





from the beginning pandemic in 2020Various containment measures were needed, such as the use of masks and social distancing, to reduce its impact. Such measures have helped “flatten the curve” and reduce the spread of the virus.
These measures indirectly affected other infectious diseases with similar transmission mechanisms. That’s why in 2020 and 2021 there was a drastic reduction in respiratory viruses in general, such as influenza (FLU), respiratory syncytial virus (RSV), HAdV, among others.
The low circulation of these viruses, in addition to the natural decrease in immunity due to previous infection, resulted in an increase in the susceptibility of the population to these agents due to newborns who have never contracted these infections. However, until recently, this did not pose a problem in the short term, as other containment measures were still in place.
With the vaccine program at the end of 2021 Covid-19 Since it has already progressed and a large part of the population is infected with the disease, sufficient robust collective immunity has been established to make restrictive measures more flexible. The long-awaited “return to normal”.
And, as expected, with increased sensitivity to other agents, these found fertile ground for proliferation. There was a peak in January 2022 H3N2 flu, Darwin variant, in a very atypical period in summer. Since the second half of 2021, there has been a significant increase in cases of respiratory syncytial virus, the main cause of pneumonia among young children.
This is where the possible relationship between the pandemic and HAdV comes into play. A significant increase in cases is expected with the expansion.
It is known that there is a strong relationship between hepatitis of unknown origin and HAdV. HAdV was identified in more than 70% of the hepatitis cases studied. The peak circulation of HAdV may be so intense that a very rare complication that goes undetected justifies these events. But we should avoid jumping to conclusions too soon. Although this virus can affect the liver of immunocompromised patients, it is not a known cause of fulminant hepatitis. We must keep ourselves open to other possibilities.
These Hepatitis Cases Are Not Caused by Covid-19 Vaccines
There are other factors to consider in this review. The first point widely reported as false or malicious is the association with viral vector vaccines for Covid-19. A thesis that can be dismissed as reason.
Coincidentally, the vector carrying the mRNA strand in vaccines such as AstraZeneca and Janssen is a human adenovirus. But each of these vaccines has a different strain than those described in the current outbreak. The virus subtype most likely associated with the hepatitis epidemic is HAdV41, while it is a recombinant chimpanzee virus used in the AstraZeneca vaccine. And it is used in Janssen’s AdV26.
In addition, the viruses used in vaccines are genetically modified to lose their replicative ability to produce spike protein (S) that creates immunity against covid-19. And what actually excludes this possibility is that most children with unknown hepatitis have not been vaccinated before.
Virus coinfections can cause
It is possible for cases of hepatitis of unknown origin to arise due to co-infection with different viruses. HAdV will be one of the candidates, perhaps in conjunction with a new variant of SARS-CoV-2. With the emergence of new variants, the emergence of re-infections was already expected. The clinical and immunological features of these variants are highly unpredictable. Omicron subvariable BA.2 is already widespread in many countries and is replacing BA.1 in Brazil (Figure 1).
Another possibility is the emergence of post-COVID-19 HAdV infection, which elicits a more severe immune response to the infection. There are 2 explanations for why cases of hepatitis are emerging now. First, the re-circulation of HAdV has only begun in the last few months. Another is that immune exacerbation may be caused by the new omicron variant BA.2.
Finally, there are several possibilities, and only through epidemiological studies, which will certainly be announced soon, can we gain more insight into the cause or causes of hepatitis of unknown origin, and with this, can we anticipate future repercussions and ways to combat it.
Figure 1 — Identification rate of each SARS-CoV-2 variant over time

Why are there no cases in Brazil?
There is not much epidemiological data on the circulation pattern of HAdV in the world. The Severe Acute Respiratory Syndrome (SARS) and Influenza Syndrome (GS) surveillance network in Brazil allows for an indirect assessment of the circulation of respiratory viruses in general. And according to Epidemiological Bulletin No. 110 There is a decrease in hospitalizations for respiratory viruses, which includes data up to April 23, 2022.
However, the decline in SARS is mainly at the expense of the decline in covid-19 As of February this year (SE7 in the table), the main cause of SARS was “other respiratory viruses”. When observing cases of influenza syndrome (GS) in Paraná, we noticed a decrease in cases (Figure 2), but a proportional increase (Figure 3) for non-Covid-19 causes.
Figure 2 — SARS cases in Brazil up to SE16

When observing cases of influenza syndrome (GS) in Paraná, we noticed a decrease in cases (Figure 2), but a proportional increase (Figure 3) for non-Covid-19 causes.
Figure 3 — SG cases in PR up to SE 13
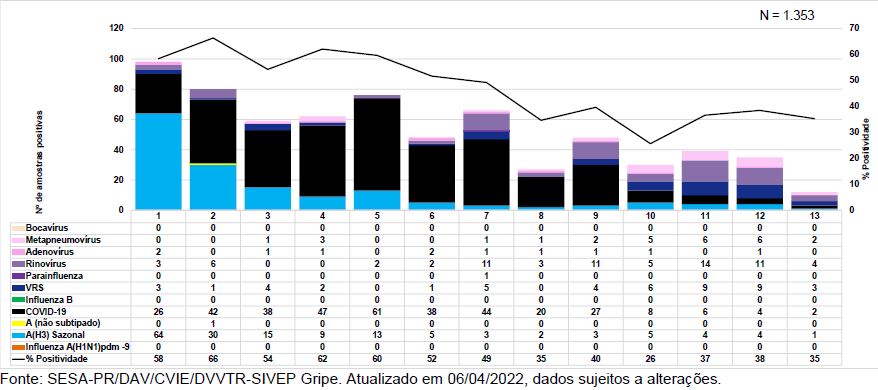
Figure 4 — Relative distribution of GS cases in PR up to SE13

The proportional increase in RSV, Rhinovirus and Metapneumovirus cases explains the significant increase in pediatric emergency/urgent care. The remaining cases of covid-19 are still at the expense of the elderly who were not vaccinated, previously uninfected and vaccinated months ago. It has also been confirmed that no significant increase so far in Adenovirus cases, representing less than 3% of GS cases in SE12 (no case detection in SE13). No data are available between SE 13 and SE19.
Given the hypothesis that hepatitis of unknown origin occurs due to some interaction between HAdV41 and the novel Omicron BA.2 variant, and that Brazil is going through a variant transition period, if there is an increase in HAdV41 cases, we will have fatal hepatitis cases. Let’s not forget that winter is coming, a time when the circulation of respiratory viruses generally tends to rise.
There are 16 suspected cases already under investigation in Brazil, but still no description allowing any assessment. If these suspicions are confirmed and new surveillance data detects an increase in HAdV circulation, the hypothesis of an association between HAdV, SARS-CoV-2 and hepatitis of unknown origin is strengthened. With the availability of more recent data and the dissemination of existing epidemiological studies in progress, we will arrive at more concrete hypotheses or conclusions.
***
Bernardo Almeida He is an infectious disease physician and chief medical officer at Hilab, a healthcare technology that developed Hilab, the first decentralized laboratory to use remote laboratory testing. He is a specialist in Infectious Diseases at the Federal University of Paraná (UFPR) and has a residency in Internal Medicine, Internal Medicine and Infectious Diseases at the Hospital de Clínicas; Master’s degree in Internal Medicine in Infectious Diseases – Epidemiology of Severe Acute Respiratory Syndrome in Adults from the same university. He has experience in infectious and parasitic diseases as well as clinical medicine. He also participates in research groups on respiratory viruses.
Source: Tec Mundo
I am Bret Jackson, a professional journalist and author for Gadget Onus, where I specialize in writing about the gaming industry. With over 6 years of experience in my field, I have built up an extensive portfolio that ranges from reviews to interviews with top figures within the industry. My work has been featured on various news sites, providing readers with insightful analysis regarding the current state of gaming culture.


: Everything we know a week after its release")


